

By Enrico Benelli
Chairperson of TDRC
E1. Why EBP and PBE matter today
In contemporary psychotherapy, two complementary paradigms guide how we understand effective treatment: Evidence‑Based Practice (EBP) and Practice‑Based Evidence (PBE). While EBP traditionally moves from research to practice, PBE brings knowledge from practice back into research.
Together, they form a circular model that strengthens both scientific credibility and real‑world clinical relevance.
The American Psychological Association defines EBP as the integration of:
- Best available research,
- Clinical expertise, and
- Patient characteristics, culture, and preferences.
This tripartite model emphasises flexibility, relational competence, and tailoring therapy to the individual.
PBE complements this by grounding knowledge in the daily reality of clinical work. It values data gathered from real clients, including those with comorbidities and complex presentations, and focuses on continuous monitoring of progress, therapeutic alliance, and global functioning.
2. Key Differences Between EBP and PBE
Enrico’s article highlights the structural differences between the two paradigms. The table below summarises these distinctions and shows why integrating both is essential for modern TA practice. This comparison shows why TA benefits from a circular integration: research informs practice, and practice refines research.
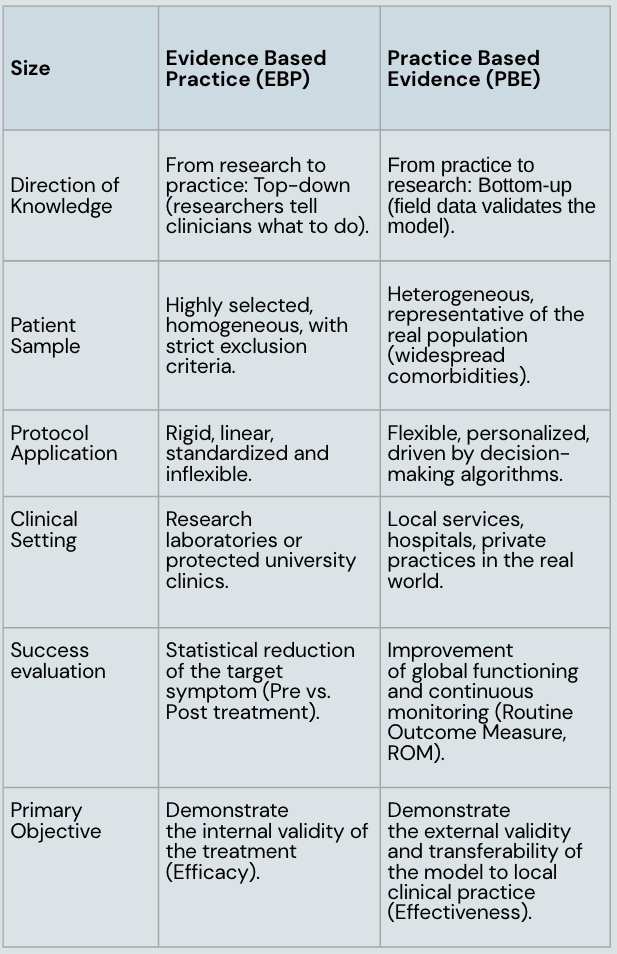
Table 1. Evidence‑Based Practice vs. Practice‑Based Evidence
3. What modern Manuals require
International guidelines (APA, WHO) now emphasise that psychotherapy manuals must be:
- Flexible and Personalised: Not rigid sequences, but adaptable principles and decision trees.
- Able to manage Complexity and Comorbidity: Real clients rarely fit a single diagnostic category.
- Process‑Based rather than Symptom‑Based: Focusing on mechanisms such as emotional regulation, self‑boundaries, and psychological flexibility.
A PBE‑oriented manual therefore includes:
- Decision algorithms to tailor interventions,
- Routine outcome monitoring (ROM) at each session,
- Fidelity and competence checklists,
- Deliberate practice exercises to strengthen clinical skill.
These elements ensure transparency, accountability, and ethical rigour; essential qualities for TA’s continued development.
4. A Contemporary Structure for TA Manuals
Enrico outlines a modern structure for TA manuals that aligns with international standards:
Chapter 1 – Theoretical Rationale and Model of Change. Conceptual framework, mechanisms of change, and supporting evidence.
Chapter 2 – Clinical Assessment and Eligibility. Inclusion/exclusion criteria, case formulation, and baseline assessment tools.
Chapter 3 – Structure of the Intervention Setting, duration, delivery format, and therapeutic contract.
Chapter 4 – Operational Guide. Flexible phases: engagement, core intervention, consolidation, and termination.
Chapter 5 – Managing Obstacles and Crises Alliance ruptures, repair strategies, and preventing dropout.
Chapter 6 – Appendices and Tools. Worksheets, monitoring diaries, clinical vignettes.
This structure supports both scientific replicability and clinical flexibility, making it suitable for real‑world TA practice.
5. Why this matters for TA
Enrico’s contribution offers a clear and timely framework for how TA can align with contemporary psychotherapy standards. By integrating EBP and PBE, TA strengthens:
- Its scientific credibility,
- Its clinical effectiveness,
- Its ethical transparency, and
- Its capacity to evolve within international guidelines.
This circular approach ensures that TA remains grounded in research while staying deeply connected to the lived reality of practitioners and clients.
For further exploration of the topic, readers are warmly invited to contact the author, who will be happy to meet and support colleagues interested in this work: tdrc.chair@eatanews.org
